Morbid obesity
Obesity is a serious chronic disease; its symptoms develop slowly and over a longer time. Obesity becomes morbid when there is a significant increase in the risk of one or more obesity-related diseases or serious diseases (also known as co-morbidities), which may lead to significant physical disability or even premature death.
Causes of Morbid Obesity
All causes of obesity are unknown. Many factors may contribute to the development of obesity, including genetic, hereditary, environmental, metabolic and nutritional disorders. Certain medical conditions can also lead to obesity, such as abnormal hormone secretion or steroid treatment.
Options for Treatment
Most conservative weight loss programs are based on dietary modifications, regular supervised physical exercise, psychotherapy, and pharmacotherapy when justified. However, it is estimated that significantly less than 5% of people who participate in non-surgical weight loss programs will lose a significant part of their body weight and maintain it for a long time. More than 90% of all people participating in these programs return to their previous weight within one year.
Permanent, significant weight loss in patients who are morbidly obese is even more difficult to achieve. This is the main reason why around 400,000 bariatric surgeries were performed worldwide in 2018. Successful patients who underwent such surgery report improved quality of life, social interaction, mental well-being, employment opportunities, and a better economic situation. Very often patients considering the surgical treatment of obesity have many serious co-morbidities and wonder if surgery is a safe solution for them. The qualification of candidates for surgery is based on very strict criteria, and only patients with an acceptable risk of perioperative complications are allowed for surgery.
Weight Loss Surgery
Bariatric surgery is a major surgery. Its growing popularity to treat morbid obesity is the result of three factors:
1) Our current knowledge of the significant health risks of morbid obesity
2) The relatively low risk of complications of the surgical procedures versus not having surgery
3) The ineffectiveness of current non-surgical approaches to achieve sustained weight loss.
Am I a candidate for bariatric surgery?
The BMI calculation helps the doctor to evaluate whether the patient will be a potential candidate for bariatric surgery. Please note that BMI is not a determining factor for eligibility or disqualification from surgery.
Bariatric surgery is recommended for people with:
– BMI above 40
– between 16 and 70 years of age
or:
– BMI between 35 and 39.9
– and one or more of the following co-morbidities:
- type II diabetes
- obstructive sleep apnea
- osteoarthritis
- high blood pressure
- high cholesterol.
BMI Calculator
Preparation for surgery
Proper preparation of the patient for surgery is an essential factor for the safe course of the procedure and uncomplicated recovery in the immediate postoperative period.
1
Psychological consultation
2
Dietary consultation
3
Consultation with doctors of different specialties, if needed:
– cardiologist
– pulmonologist
– endocrinologist
– anaesthesiologist
– other
4
Esophagogastroduodenoscopy, EGD
5
Laboratory tests: Morphology, sugar level, glycated haemoglobin (HbA1c), iron level, transferrin, TSH, FT3, FT4
6
Abdominal ultrasound
7
7% reduction in initial body weight
8
The Questionnaire on the Surgical Treatment of Obesity
Please complete the questionnaire. The answers will make it easier to qualify the patient for the surgery. Sendng back the questionnaire is not obligatory, but failure to do so, may prevent the provision of medical services.
Types of Bariatric Surgery
Several different types of bariatric operations are currently being performed in specialized clinics. Many factors are taken into account when selecting the type of surgery, including initial body weight, co-morbidities, risk assessment, and age of the patient. Before the operation, the surgeon will explain to the patient what are the different procedures and indicate which operation will be best for him.
Bariatric operations performed in our hospital:
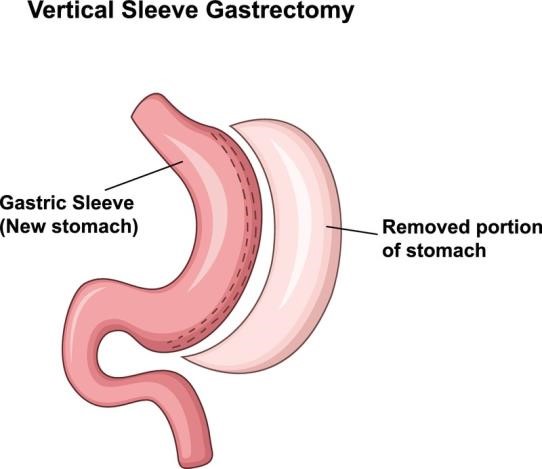
SLEEVE GASTRECTOMY
Sleeve gastrectomy has become in recent years the most common bariatric operation in the world. It is performed under general anesthesia. A laparoscopic technique makes the surgery minimally invasive and enables patients to recover quickly.
This is a restrictive procedure and consists of removing about 80-85% of the stomach volume. As a result of reducing the stomach capacity to about 130-150 ml, the patient limits the amount of food taken at one time.
During the surgery, the part of the stomach that is responsible for the production of ghrelin, i.e. the hormone of hunger, is removed, which leads to its lesser secretion and, as a result, to a decrease in appetite and feeling of hunger. Since this operation is performed only on the stomach, the food delivered in a limited volume passes through the remaining intact part of the digestive tract and is digested and absorbed physiologically.
GASTRIC BYPASS
Gastric bypass is also one of the most common bariatric procedures in the world. The procedure combines both restrictive and malabsorptive components. In this operation, the stomach is not removed. A small gastric pouch with a volume of about 25-30 ml is created from the upper part of the stomach. Food will be delivered only to this small, separated part of the stomach from which it will be rerouted directly to the intestine. Food will pass a much shorter route through the intestine than before. It will bypass the entire stomach, duodenum and a considerable part of the small intestine. This means that in addition to reducing the volume of the stomach, the digestive part of the gastrointestinal tract is also shortened, which reduces the absorption of food ingredients.


MINI GASTRIC BYPASS
Mini gastric bypass is also an effective laparoscopic bariatric procedure recommended for obese patients, usually with coexisting diabetes, hypercholesterolemia and uncontrolled hypertension.
This procedure consists of dividing the stomach and creating along its smaller curvature a fairly long but narrow food pouch which is then joined directly to the small intestine in such a way that the route the food takes through the digestive tract is about 200 cm shorter than before.
Mini gastric bypass, similarly to gastric bypass, is both a restrictive operation and one that ensures incomplete absorption of the consumed food. A gastric pouch is quickly filled with a small amount of food resulting in an early feeling of satiety.
BARIATRIC SURGERY REVISION:
– LAP-BAND® Surgery Revision
– Gastric Sleeve Revision
– Gastric Bypass Revision.
A hospital stay after a revision bariatric operation takes a day or two more than after the initial surgery because it is an operation with a higher risk of complications and the patient requires longer medical surveillance. During these surgeries, the surgeon operates on scarred tissues, with impaired blood circulation and inferior healing capacity.
After leaving the hospital, most patients return to health and normal life within a few weeks or so.
Risks can include:
- longer surgery time
- the possibility of converting a laparoscopic operation into a classic one during the procedure
- higher blood loss
- infection
- leaks.
Life After Bariatric Surgery
Bariatric surgery is not a miraculous remedy for obesity, but rather a powerful tool to help you lose weight to be healthier and enjoy a longer and more satisfying life. Long-term improvement after the operation depends on following the guidelines for diet, exercise and lifestyle modification.
When you leave the hospital, you will receive prescriptions for several medications. Some of these medications will be taken for a few months after surgery, and others you will take for life.
Don’t take non-steroidal anti-inflammatory drugs (NSAIDs) such as asprin, ibuprofen, and the like. These medications increase your risk of developing ulcers.
The following vitamins and minerals should be taken daily to prevent postoperative nutritional deficiencies:
Multivitamin supplements
Take daily multivitamins and minerals containing a minimum of 18 mg of iron, 400 mg of folic acid as well as selenium, copper, and zinc.
Calcium
Take 1,200 to 2,000 mg daily to prevent calcium deficiency and bone disease. To increase absorption, take calcium supplements in two or three divided doses per day. Calcium citrate is the preferred calcium formula.
Vitamin D
Take between 800 and 1000 International Units (IU) of vitamin D per day. This total should be taken as 400-500 International Units (IU) twice a day with added calcium.
Vitamin B12
Take 500 mg of vitamin B daily. It can be taken as a tablet, sublingual tablet or liquid. Remember that the whole tablet must be crushed.
You may need additional supplements of folic acid or iron, especially for menstruating women.
Women of childbearing age are not recommended to become pregnant within two years of having a bariatric operation. A pregnancy that develops during this period can lead to damage to the fetus and congenital defects.
The time of the patient’s return to work depends on his general state of health and physical condition before the operation. Many patients return to work two weeks after the operation, without any activity limitations. However, some need an additional two weeks. Return to full physical fitness is different for each individual and usually takes about six weeks.
After the procedure, the dietician prepares a dietary plan for the patient, which must be strictly applied. For a certain period it may be a liquid diet, followed by a transition to soft or mashed food, and finally to solid food.
It is very important to provide enough fluids to the body. The goal should be to drink 1.5 to 2 l or more of fluids per day to avoid dehydration, constipation and kidney stones.
Nutritional guidelines limit the number of calories consumed while providing balanced meals to prevent nutrient deficiencies and preserve muscle tissue. Each patient tolerates the recommended diet differently.
A low-calorie, low- fat and low- sugar diet is recommended. The aim is to provide at least 65-75 g of protein per day. High-protein foods include eggs, meat, fish (tuna), seafood, poultry, milk, soy, cottage cheese, and yogurt. Do not worry if you do not achieve this amount of protein in the first few months after the operation.
Here are some eating guidelines:
– Eat slowly and chew small bites of food thoroughly.
– Avoid rice, bread, raw vegetables, fresh fruits, and meats that are not easily chewed such as pork and steak. Ground meats are usually better tolerated.
– With soft and solid foods, take only three bites at one sitting, then wait a minimum of 20 minutes before eating more.
– Eat balanced meals with small portions.
– Avoid the use of drinking straws and carbonated beverages, chewing gum and ice because they can introduce too much air into your pouch and cause discomfort.
– Avoid sugar, sugar-containing foods and beverages, concentrated sweets, and fruit juices.
Over time, increase the variety and consistency of the foods in your diet. Some foods may be poorly tolerated initially such as red meats, chicken, breads, high fiber fruits and vegetables. This will improve over time.
It is very important that you stay well-hydrated; you should drink around 1.5 to 2 litters of fluids daily, unless otherwise restricted by a medical condition.
Alcoholic beverages will have a more profound effect and should be avoided or consumed with caution.
It is recommended to exercise for 30 to 45 minutes a day, at least three times a week.
Initially walks are recommended and then you can introduce exercises such as jogging, swimming or riding a stationary bike.
Costs
| No. | Name of the medical procedure | Abbreviation | Price |
|---|---|---|---|
1. | Laparoscopic sleeve gastricectomy (procedure) | BAR1 | 18 900,00 PLN |
2 | Laparoscopic Gastric bypass | BAR2 | 22 500,00 PLN |
3. | Hospitalization at the Department of General and Transplant Surgery – 1 day | BAR3 | 1 450,00 PLN |
4. | Dietary consultation along with nutritional recommendations | BAR4 | 310,00 PLN |
5. | Dietary consultation | BAR5 | 230,00 PLN |
6. | Individually developed 7-day menu | BAR6 | 210,00 PLN |
7. | Medical consultation (Obesity Treatment Center) | BAR7 | 255,00 PLN |
8. | Psychological consultation | BAR8 | 230,00 PLN |
Team
Bariatric Surgery at the Clinical Hospital No. 2 of the Pomeranian Medical University in Szczecin, Poland